Oral Health is Important to Pregnancy
The Michigan Maternal and Infant Oral Health Project (MIMI-OH), funded by the Michigan Department of Health and Human Services (MDHHS), integrates registered dental hygienists (RDH) within an obstetric setting to provide care efficiently as part of an inter-professional team. This project is a coordinated partnership involving the University of Detroit Mercy, the MDHHS Oral Health Program, and the Michigan Primary Care Association. Grace Health was our model site and clinical consultants.
Improving Workflow
How can we provide more dental assessments for pregnant women?
“Incorporating a dental assessment into either the intake appointment and/or the first physical would definitely increase the number of assessments and save hygienists a lot of leg work. However, the known barrier of limited time remains an issue. Some providers find that the length of the intake visit is already long, leading to the perception that adding a dental assessment to those visits would add too much time to the patients’ appointments. Usually, the hygienist greets the patients in the waiting room or exam room and introduces herself and the oral health services offered through this program. After the introduction and patient education, hygienists have been scheduling out the next prenatal visit along with either an hour or ½ hour hygiene visit as patients walk out the door.” – Stacy Hofmeister, RDH, Ingham County
How can we improve access to dental care for pregnant women?
“I am educating and referring every single patient every single time.” – Staci Hard, RDH, Grace Health
Initial Pilot Site Impact
As of mid-May 2018, our 5 active pilot sites reported seeing 729 pregnant patients, measured through Patient Education provision (D1330). Of those, 69% received an Oral Assessment (D0191) and 58% were referred to a dentist.
The project officially launched in Oct-2017 when Dr. John Girdwod was hired as the statewide program manager. Data for Oct-2017 through Dec-2017 were reported solely from Grace Health, our model pilot site, whose Registered Dental Hygienist (RDH) logs about 24 hrs/wk during a normal month. This equates to a benchmark, measured in Oct-2017, of 1.8 hours of dedicated RDH work time per patient. We will measure that again for all sites at the end of the grant period to look for any changes or trends.
By our 6th month (Mar-2018), our 5 active sites averaged just over 33 patients per month, measured by the count of D1330 Patient Education provided to patients. This is exactly how many patients Grace Health’s RDH saw on average, per month, during our first 3 months. During subsequent months, we will examine the feasibility of seeing > 33 patients per month at each site.
Click here for more information about our sites!
Pilot Site Performance
This project began in Fall 2017 with the goal of implementing oral health services at 6 pilot sites throughout Michigan. Although our sites share similarities, e.g. they are all FQHCs, they function a little differently across the state. We tried to standardize work when we could, but we emphasized each site’s strengths so that shared knowledge would help improve workflow.
The following snippets include some data and are meant to convey narratives, or “tell the story,” about how sites implemented this MDI project in their clinic.
Grace Health
Our model pilot site, Grace Health in Battle Creek, set the tone for this project. Their site RDH, Staci Hard, is employed part-time at 24 hrs/week so we examined initial benchmark KPI off that knowledge.
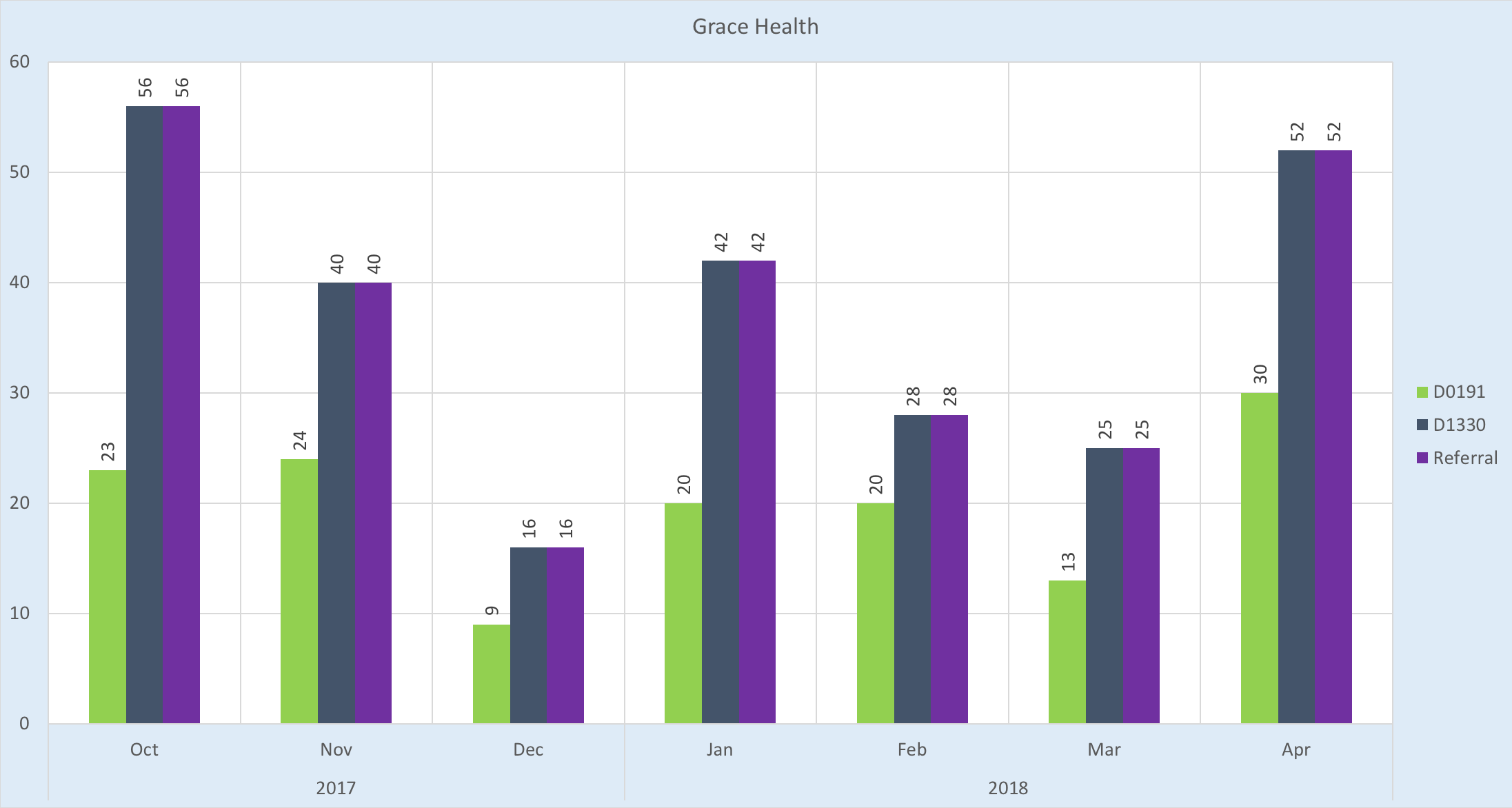
The strengths at Grace Health are (1) stability of the project; (2) cultural integration; and (3) every patient is referred to a dental home. Referrals are structurally fluid due to the dental clinic’s close proximity (a matter of feet) to the OBGYN clinic and culturally successful because Staci Hard, RDH has made referrals standard work.
Ingham County Health Department
Our model government-run health clinic, Ingham County Health Department Women’s Clinic, launched somewhat late in the 1-year grant timeline but immediately began maximizing the hygienist’s time, serving the most patients of any site employing a full-time hygienist.
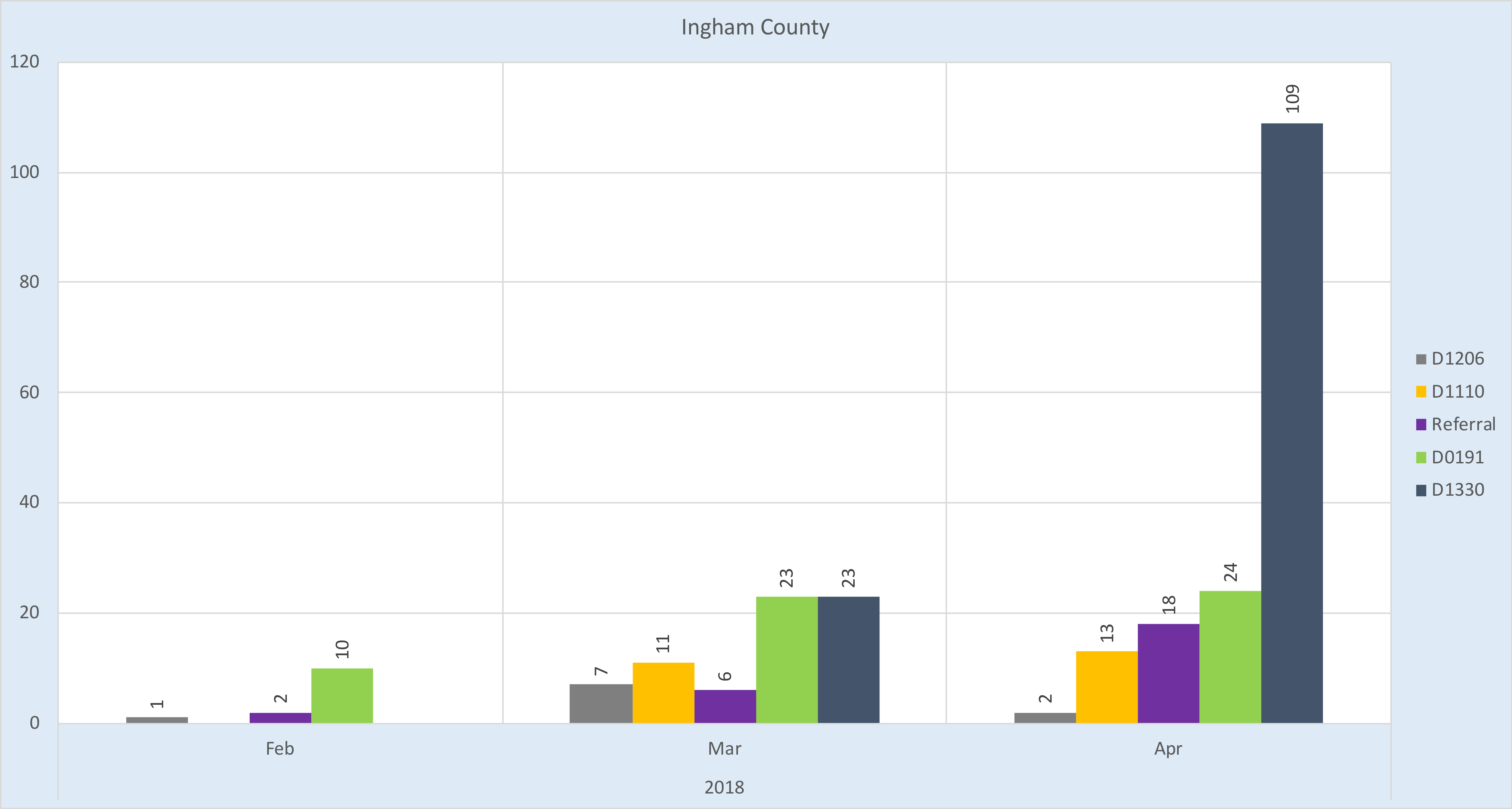
The strengths at Ingham County are (1) maximized RDH time; (2) cultural integration; (3) ability to provide patient care like prophylaxis and fluoride varnish; and (4) integrated OBGYN and PED care. Integrated PED care is structurally fluid due to the dental clinic’s close proximity (a matter of feet) to the PED clinic and culturally successful because Stacy Hofmeister, RDH has made seeking PED patients standard work. Additionally, Connie Crowe supervises both PED and OBGYN clinics so there is universal oversight of care for both pregnant women and children, involving the entire family as a unit of care.
Great Lakes Bay Health Center
Our model stand-alone health clinic, Great Lakes Bay Health Center, launched somewhat late in the 1-year grant timeline but immediately began making quality improvements as shown by the upward trend each month in patient care.

The strengths at Great Lakes Bay Health are (1) continuous improvement and (2) cultural integration. Continuous improvement is supported by Paul Crowley, DDS, who makes regular trips from the health system’s off-site dental clinic to the OBGYN health center. Additionally, Leanne Jordan, RDH works diligently to think of new ways to reach patients like placing a “DENTAL” sign outside the room door, adding posters throughout the clinic to promote the program, and seeking micro-time slots during which she can see patients. She locates available patients who are waiting in empty clinical rooms through a room flag system. Cultural integration is supported by Doug Saylor, MD, who is both Medical Director for the health system and an OBGYN physician.
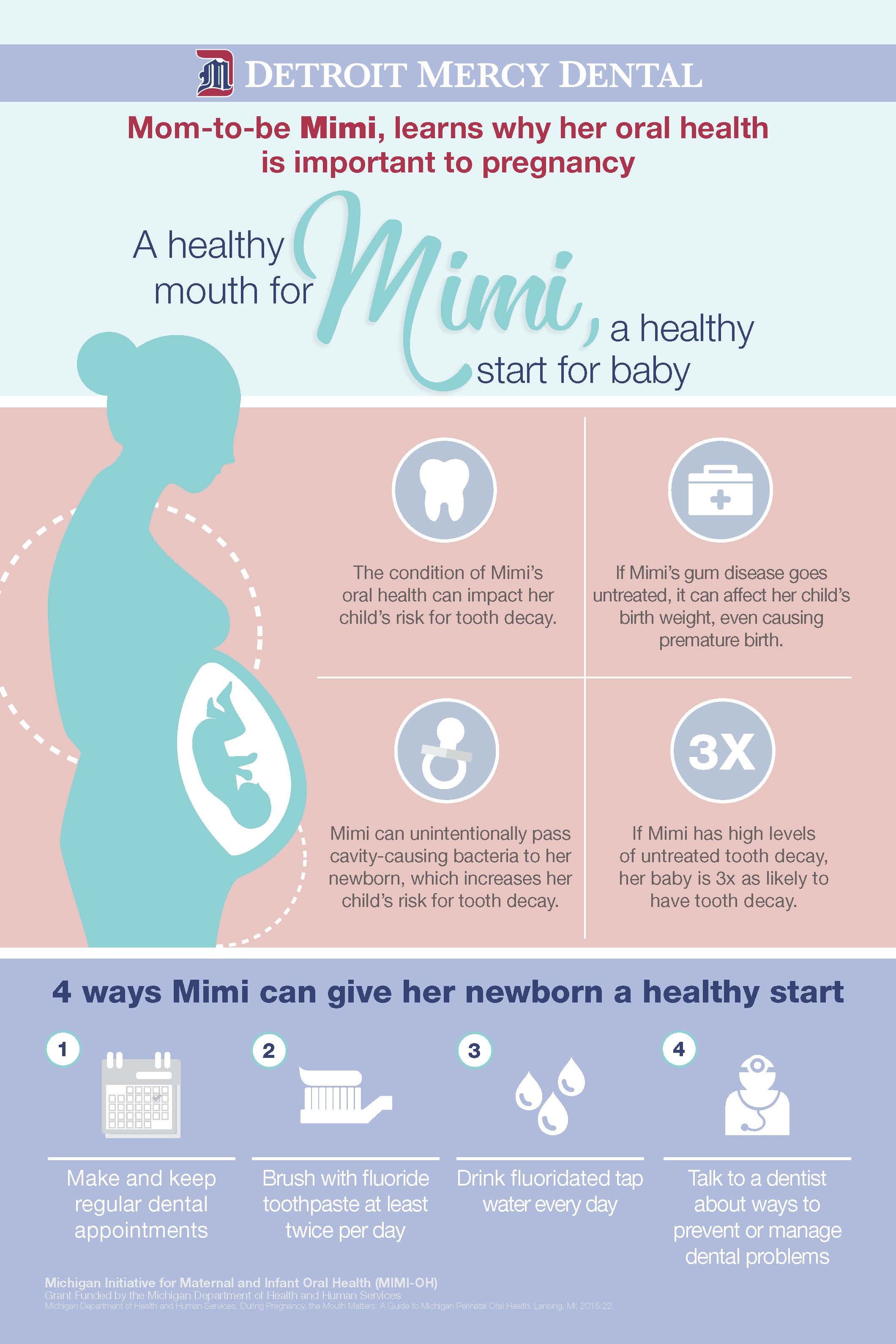
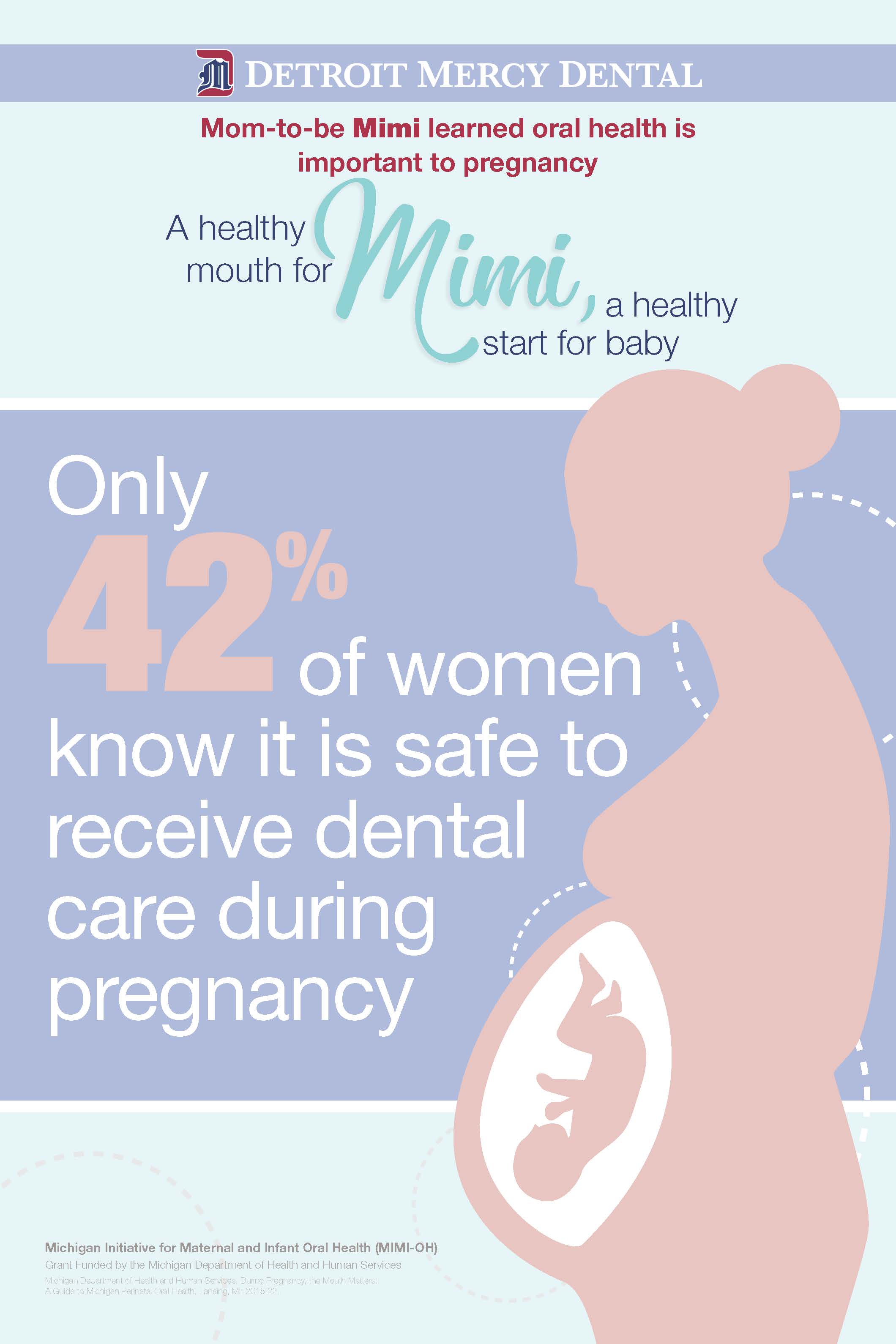
Promoting Oral Health During Pregnancy
Click here for PDF of all the poster images you see below or click on each individual image to get a high resolution JPEG of that image. Questions about use should be directed to Dr. John Girdwood, Statewide Project Director at girdwojr(at)udmercy(dot)edu. Free to use and copy for all project sites!
The Michigan Maternal and Infant Oral Health (“MIMI-OH”) project was launched in 2017 and has continued to grow statewide. Our goal is to improve oral health outcomes for mothers and infants through quality medical-dental integration. We define quality care as being safe, timely, effective, efficient, equitable, and patient-centered. Our project places a Registered Dental Hygienist into an OBGYN medical clinic through Michigan’s PA161 program. We have sites in Bay City, Benton Harbor, Muskegon, Battle Creek, Lansing, and the Upper Peninsula.

Initial Impact (Documented)
- 469 patients have received an oral assessment*
- 75 patients have received a dental cleaning*
- 36 patients have been referred to a dentist*
- 77 patients have received oral health education*
- 26 patients have received an oral evaluation exam*
- 1 child received fluoride varnish treatment*
- 123 patients have participated in a saliva-check research study*
* These numbers were provided to us by our clinical sites, are based on care recorded in the electronic dental record (EDR), and may not include data from all sites. You can read about the EDR codes we use by clicking this link. Data were updated: 03/28/2018
Project Team

Health Mouth for You = Healthy Start for Your Baby!
